
Exploratory Laparotomy Set Up

Here’s what I put on my mayo stand for an exploratory laparotomy with a little explanation. What I put on the mayo is highly reflective of who the surgeon is and what the potential procedure will be. In this instance, it was an abdominal stabbing with bowel involvement. First, I always start with a #10 scalpel on a #3 knife handle for the first incision. After that incision is complete, I place it on the back table to avoid a sharps injury. Next, I throw up a few pick-ups- my go to is usually a few DeBakey forceps of different lengths. Then a variety of scissors- Metzenbaum, straight Mayo, a long Metz, and a long Mayo. The patient’s size determines how many of these I will usually start with on my mayo. If the patient has a high BMI I will put up the long Mayo, however if they have an “average” or low BMI, I will just stick with the regular length Mayo scissors. I recogniazed that not very many of the surgeons I worked with wanted to use the long Mayo scissors- so I stopped putting them up all the time! But, this patient did have a high BMI. Then on my instrument roll (I will never understand the anti-roll techs!) I always start with 4 Kellys, 2 Kochers, 2 Allis (they are hidden behind the Kochers in this picture), 2 long Allis, 2 long Babcocks, 2 Babcocks. I also usually put a long-ish right angle, or Mixter, up on my instrument roll, I must have forgotten to pull it up this day! Then over to the side of the instrument roll I have two Ring Forceps (or what people call sponge sticks, but they aren’t technically sponge sticks until you put the Raytec on them! This might be a pet-peeve of mine). Then a medium sized Richardson retractor. Typically, I would put up a few other handheld retractors, but this surgeon goes straight to the Bookwalter for most abdominal procedures. I also have a set of lap sponges up on the mayo. If this was an unknown injury, I’d likely have 1-2 more sets of laps up on the mayo. Under the first towel I have a few different sets of silk ties readily accessible- these ones are 0 and 2-0.

INTRAOPERATIVE TIP
INTRAOPERATIVE TIP
For all exploratory laparotomy cases you should always have the GI staplers and reloads readily available. Check out my guide for GI staplers here.
INTRAOPERATIVE TIP
INTRAOPERATIVE TIP
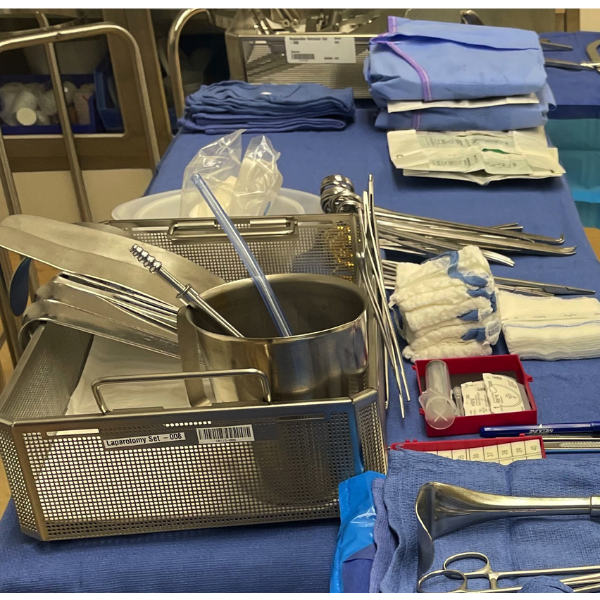
Now for the back table! If you can’t tell, I prefer a condensed table. I like to condense my table because it allows me to reach for things without stepping back from the field, but it also allows me to have room to add things as needed- which is sometimes done urgently, and I don’t have time to make room! I like to put my instrument pan on the back corner of the table but empty the ringed instruments out. I was taught in school to put the instrument tray in the back center of the table, but that just did not make sense to me, so I adapted it to what made sense for me. Again, this helps me reach what I need without stepping away from the field. I open up an extra Poole suction and an extra Yankour suction for each belly case because you never know when you’ll quickly need another due to a contamination. I like to slip those both into the pitcher for easy access. I place the pickups on the front panel of the instrument tray, UNLESS they are fine pick-ups. For those I lay them out on the table, so they are not damaged. I put all of the handheld retractors “on display” leaning against the back panel of the instrument tray. This allows me to easily see and grab what the surgeons needs quickly.
In front of the instrument tray, I put my sharps box. I like to separate mine and create a small space between where I put my extended bovie tip, a 15 scalpel on a #7 handle, then a marker. Doing this helps me keep a safe place for the other scalpel. Then, I place other half of the sharps box and store miscellaneous items in here- pictured is a 10cc syringe and 2 #1 looped PDS. This is *NOT* an appropriate place for any suture that is smaller if there is a magnet in the bottom as it can become magnetized and that’ll really make the surgeon real happy! If I had smaller sutures opened, I would arrange them in front of the box, or stack them in a med cup, it really just depends on what suture I have open and how much! Next to that I put my additional sponges. Sometimes I will put extra laps in the instrument tray where the pitcher is and move the pitcher back. Beside that is another instrument roll (Yes, another!) with the rest of my instruments. I always start this (from left to right) with scissors then needle drivers, then I leave a small gap and start with the rest of the ringed instruments. I usually try to mimic the order of the count sheet- it makes counting MUCH smoother. Behind those I have some of the items that come in the pack that I may not be using right away or at all. If the pack doesn’t have a trash bag, I like to use the round basin as a trash can and the kidney basin will be saved for if/when we staple the bowel. On the far side of the back table is the additional towels and gowns and gloves for the rest of the team, and usually at least one extra gown and always an extra set of gloves for the surgeon.
Then on the second table I have just the Bookwalter retractor. Usually, I open this onto the primary back table, but our trauma room is an “ortho” room meaning… extra tables, so why not! I like to organize this in the order use, and I keep all of the parts that are not usually used in the instrument tray. If I have it on my primary back table, I would lay a blue towel over the non-used items (after counting of course!) and then organize the clamps and arms in the tray.

The last thing (which is actually the first thing I end up setting up) is the ring stand. I use the ring stand for everything to drape the patient and things that will be thrown off the field. Everything that is placed on the patient is put into this basin backwards or upside down to make draping the patient a smooth process! In this basin I have the skin prep (Chloraprep), four towels to “square off” the field, the laparotomy drape, an Ioban pouch (best invention ever!), suction tubing with tip attached already, the bovie in the holster, the Ligasure Impact, and last is light handles!
Now, this is tailored to the surgeon performing the procedure so there are some things added or missing. For example, I do not have any bowel clamps up on my mayo, they are on the back table on the instrument roll on the very end. I would usually have those up on the mayo for any open belly with a potential for bowel resection- however, this surgeon doesn’t use them. Also, you may have though my mayo stand was set up backwards, but it’s not! As a new tech I got into the habit of turning my mayo stand around after draping so I was looking at it as I was standing where I would be during the procedure- this helped me be more efficient in my set ups and it just stuck with me!
Here are a few things that helped me be more efficient with my set ups… Try to put things in the same place (or as close as possible) for each set up. Try not to move things multiple times, if you pick it up- put it in its final place. I know that sounds self-explanatory, but when you take a back table pack with everything packed up into one small area and multiple instrument trays and turn it into this, sometimes it’s easy to grab things at the wrong time and end up having to move it multiple times. It’s like a big puzzle! I love to organize a back table and mayo stand, and really anything! No wonder I enjoy this field so much!
What are some of your set up tips? What helped you with your set ups? I hope this was helpful!