
Septoplasty with Inferior Turbinate Reduction
What is a septoplasty?
A septoplasty is a procedure targeting at repairing or straightening the deviated septum, the portion of bone and cartilage between your nostrils. There is a small incision made on the septum inside the nostril.
What is a turbinate reduction?
First, what’s a turbinate? These are the nasal concha- they help to regulate air flow through your nose. When you have that “stuffy” feeling, it’s usually your turbinates being enlarged inhibiting your desired airflow on inhalation. These can become permanently or chronically enlarged. This portion of the procedure is aimed at reducing the size of the turbinates within the nasal cavity in order to promote better airflow to improve breathing.
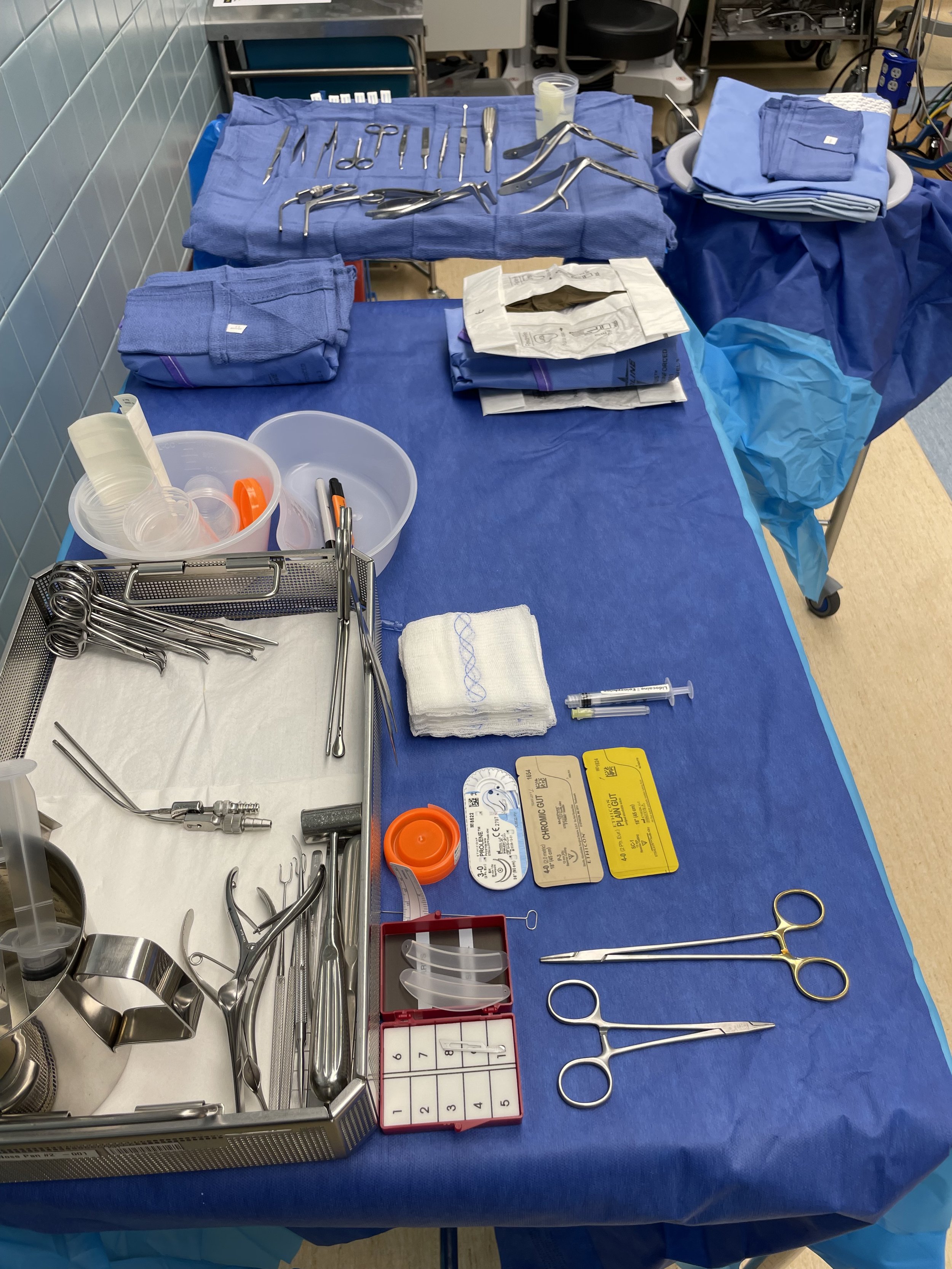
These procedures are fairly quick and don’t require too much instrumentation or set up. The surgeon will need a headlight and will inject local with epinephrine prior to draping, doing so will allow for the epinephrine to help reduce bleeding during the procedure. Below is what I have available for a straightforward Septoplasty with turbinate reduction.
On the Mayo:
11 blade on a #7 knife handle
Adson tissue forceps
Bayonet tissue forceps
Curved Iris scissors
Straight Iris scissors
D-knife
Button knife
Freer elevator
Cottle
Nasal fracture elevator (AKA Butter knife)
Cup with saline and instrument wipe
Double action scissors
Double action ronguer
Nasal specs (various sizing)
Takahashi (Whatever forcep the surgeon will use to remove tissue/septal fragments)
Frazier suction (1 already up on the suction tubing)
Cottonoids (1/2” x 2”) tucked underneath the towel

On the Back Table:
Nose pan and contents
Needle board; 15 blade to swap out for the 11 after initial incision. I also put the Doyle splints for end of the procedure here. Right beside the needle board I put the brush for cleaning the microdebrider tip. Then an upside down med cup where I will have the nurse put the bacitracin that I will coat the Doyle splints with closer to the time of use. Below that I have the Prolene that the Doyles are sewn in with- it’s a double armed suture, but one needle is cut off. Then chromic and plan gut for closure. I always keep an extra 3cc of local (typically 1% lidocaine with epinephrine 1:100,000) with a 27g hypodermic needle incase the surgeon chooses to inject more local. Raytecs- which typically are only used for cleanup during a septoplasty.
In the basin:
Light handles (not a real need, but our packs come with them)
Suction
Microdebrider
Clamp to secure to drape
ENT Split drape
3 towels (one across ET tube, two to place from outer lip to between eyebrows)
Depending on the surgeon’s preference, you may or may not use Doyle splints- they help to keep the nares open and patent during recovery and provide a firm(ish) structure against the newly repaired septum. You may or may not use a bandage which is typically an “eye” bandage placed below the nose folded in half and secured with paper tape- nothing fancy! Patients will go home the same day typically, they may have bleeding for the first few days, but after that they should be feeling pretty good.
Some surgeons still use the osteotomes and mallets for this procedure, luckily for me this wasn’t the standard with the surgeons I worked with – I don’t know why but that part just gives me that cringy feeling!